|
Interesting Clinical Cases - Prenatal diagnosis of Mesoblastic Nephroma associated with polyhydramnios: a case report Prenatal diagnosis of Mesoblastic Nephroma associated with polyhydramnios: a case report.
Website: www.drnayansarkar.jivisha.com Blog: www.drnayan.blogspot.com
Introduction Fetal kidney tumor is an extremely rare phenomenon in clinical practice and diagnosis of it antenataly is exceptional. The sonographic feature of the surrounding structures makes it difficult to image both kidneys satisfactorily. Most of the kidney diseases are cystic and obstructive type of nephropathy associated with oligohydramnios[1].Only few cases diagnosed by prenatal ultrasound have been reported so far in world literature .This present case report elucidates sonographic features of a Mesoblastic Nephroma with polyhydramnios at term in labour and formulates a brief discussion. Case report A 20-years-old primigravida presented
to our Emergency Obstetrics Services at term with concerns
of suspected rupture of membranes and leaking of amniotic
fluid in early labour. As there was no obvious leakage of
fluid, an emergency ultrasound was performed and severe
polyhydramnios was visualized which guided to perform a
detailed ultrasound examination. A detailed appraisal
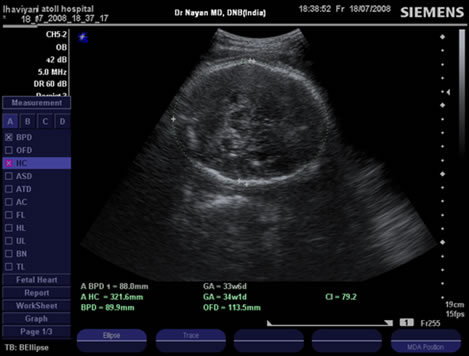
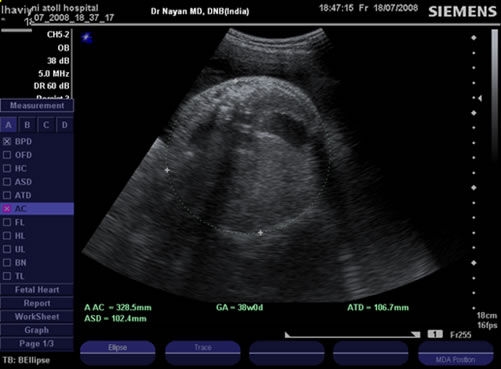
revealed an abdominal circumference significantly greater
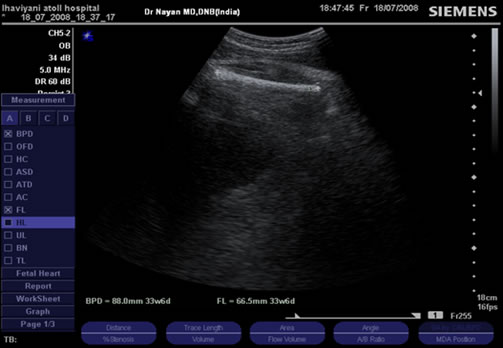
than other biometric measurements.BPD, HC, FL were
concurring to 34 weeks of gestation whereas abdominal
circumference showed 38 weeks. Presence of an
intra-abdominal solid tumor with well defined borders that
displaced the fetal liver cranially was noted. The size of
the tumor was 7.5×6.9 cms. The normal appearing left kidney
was noted but the right kidney could not be identified. It
was a male fetus with normal appearing bladder and urethral
region. Based on these findings of solid renal mass and
associated polyhydramnios a Congenital Mesoblastic Nephroma
was proposed as possible diagnosis. There was no history of
maternal diabetes. It was a non consanguineous marriage. As
patient went into active labour and could not tolerate pain
a caesarean section was performed at maternal request.
Neonate was born with a good Apgar score and examination
revealed a huge solid mass occupying almost the whole right
side of abdomen. Baby had neonatal problem of transient
respiratory difficulty and jaundice which got settled .CT
scan abdomen revealed a neoplastic lesion arising from mid
and lower third of right kidney and extending abdominal
quadrants. No vascular invasion was noted and a diagnosis of
Mesoblastic Nephroma was suggested. The neonate was operated
in India two weeks after birth .A right sided
nephrouretrectomy was done .Right kidney was totally
replaced by a solid tumor of 7.5×6.9 cms, with round and
well defined borders, the cut surface was yellow-grey, firm,
rubbery in consistency. His postoperative period was
complicated by mild feed intolerance and suspected sepsis
which was managed by IV antibiotics. Histopathology
confirmed the diagnosis of Mesoblastic Nephroma. Microscopy
revealed interlaced bundles of fibroblast and myofibroblast
with eosinophilic and fibrillar cytoplasm and round to oval
nuclei. There were focal areas of immature cartilage and
dysplastic glomeruli and tubules. Sonography:
Polyhydramnios –the first clinical clue of many congenital anomalies, though most renal anomalies are associated with oligohydramnios.
Solid mass of 6.9×7.5 cms. in abdomino-pelvic area
Fetal biometry- both BPD & FL show gestational age of around 33-34 weeks.
Disproportionately advanced gestational age of 38 weeks by abdominal circumference because of intra-abdominal mass.
Discussion
To differentiate a Mesoblastic Nephroma from Wilm’s tumor we need histopathology, but it is true that Mesoblastic Nephroma have been diagnosed more frequently in utero. In infantile polycystic kidney disease there will be bilateral renal enlargement and oligohydramnios with non visualization of fetal bladder. In diffuse nephromatosis [9] both kidneys are involved and may show acoustic shadowing due to calcification. Kidney enlargement in some inherited disorders such as Meckel's syndrome is generally bilateral. Solid tumor arising in paravertebral area from adrenal gland or extrathorasic pulmonary sequestration can be distinguished from renal tumor by the presence of a normal appearing kidney in that area. Severe polyhydramnios may necessitate periodic amniocentesis to prevent preterm labour for polyhydramnios. Antenatal steroid should be given thinking that polyhydramnios may lead to prelabour rupture of membrane and preterm labour and delivery. If diagnosed early a serial ultrasound to evaluate tumor growth and fetal growth should be performed and a thorough search for other associated anomalies as well. Isolated congenital Mesoblastic Nephroma carries an excellent prognosis after neonatal surgery is performed, and hence ruling out of any other anomalies is so important. Unless dystocia because of huge fetal abdomen is anticipated caesarean delivery per se is not a requirement. Although it is desirable to arrange delivery of such a case in an equipped hospital with facility to do pediatric surgery situation may arise as we had to deliver her by caesarean and then refer to abroad. Even though most patient will be cured and do excellent after nephrouretrectomy [10] periodic follow up should be scheduled and followed as our case is following.
References: 1. Callan NA, Blakemore K, Park J, et
al: Fetal genitourinary tract anomalies: Evaluation,
operative correction, and follow-up. Obstet Gynecol
75:67-74, 1990. |
||||
|
|
||||